






When a newborn struggles to breathe after birth, many things must be considered, and persistent fetal circulation / persistent pulmonary hypertension in the newborn (PPHN) is one of them. PPHN means that the pressure in the blood vessels supplying the lungs remains high, and this leads to problems.
In babies with PPHN, certain blood vessels that remain closed during gestation do not open up properly after birth to allow blood flow to the lungs. This can result in a very dangerous situation where the baby is not able to start breathing independently, often requiring emergency neonatal resuscitation. Medical malpractice involving PPHN usually involves a failure to properly respond to and manage babies in need of respiratory support.
The birth injury attorneys at Miller & Zois can help you investigate your PPHN case and pursue any potential claims for medical malpractice. Call us for a free consultation at 800-553-8082 or submit an online contact form.
PPHN
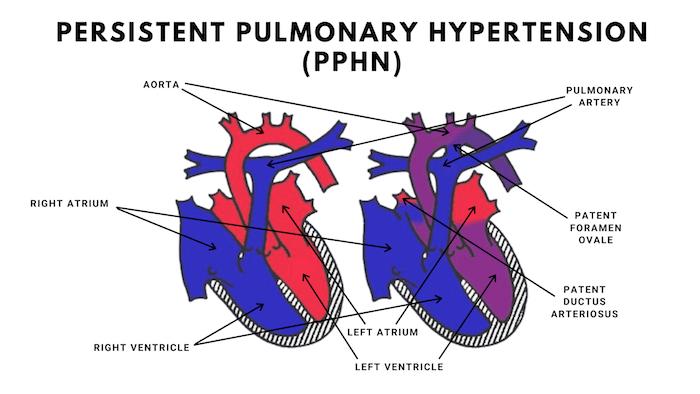
PPHN is fundamentally a disorder of the lungs and the cardiopulmonary system. Before birth, a baby does not use the lungs to breathe. Oxygen is delivered through the placenta, and the fetal circulatory system is designed to bypass the lungs almost entirely. Because the lungs are still developing and filled with fluid, the blood vessels within them remain tightly constricted. Most of the baby’s blood is diverted away from the lungs through specialized fetal shunts, including the ductus arteriosus and the foramen ovale, which route blood directly back into the systemic circulation.
At birth, this system is supposed to change within minutes. When a newborn takes the first breaths, air fills the lungs and oxygen levels rise. That rise in oxygen triggers the pulmonary blood vessels to relax and open. As those vessels dilate, blood begins flowing through the lungs to pick up oxygen and release carbon dioxide. At the same time, the fetal shunts begin to close. This coordinated transition allows the baby to shift from placental oxygenation to independent breathing.
In babies with persistent pulmonary hypertension of the newborn, this transition fails. The pulmonary blood vessels remain constricted instead of opening. Pressure in the lungs stays abnormally high, and blood continues to bypass the lungs through the fetal pathways. In other words, circulation partially reverts to the fetal pattern even though the baby is now outside the womb. That sustained high pressure in the pulmonary arteries is what gives the condition its name.
The consequences are serious and immediate. When blood is shunted away from the lungs, oxygen cannot adequately enter the bloodstream. The baby may appear blue, struggle to breathe, or require aggressive respiratory support. Without sufficient oxygen exchange, every organ is at risk. The brain is particularly vulnerable. Even short periods of oxygen deprivation can lead to hypoxic-ischemic injury, permanent neurological damage, or death.
PPHN Occurrence and Risk Factors
PPHN is a very uncommon condition, occurring in about 1 out of every 500 babies. PPHN can be a very serious and very dangerous condition for a newborn. Approximately 17.5% of children with PPHN die and many more suffer brain injuries, hearing deficits and permanent lung injuries.
PPHN is associated with term or post-term infants, usually after a difficult birth. Risk factors associated with PPHN include meconium aspiration, birth depression, maternal infection, and congenital abnormalities of the heart or lungs. There is also an association with mothers who took certain medications such as nonsteroidal anti-inflammatories and certain antidepressants.
PPHN Symptoms & Treatment
The signs of PPHN include rapid breathing, grunting or moaning sounds, poor skin color, low oxygen levels, and low blood pressure. These symptoms are often identified shortly after birth using an APGAR test.
When clinical signs of PPHN are present, confirmation is typically made with an ultrasound of the heart, known as echocardiography. This is considered the most reliable noninvasive test for establishing the diagnosis. Prompt diagnosis is critical because babies with PPHN frequently require immediate and aggressive medical intervention.
Initial treatment focuses on stabilizing the infant. This includes keeping the baby warm, administering antibiotics if infection is suspected, and providing supplemental oxygen. Oxygen may be delivered through a mask, oxygen hood, or small tubes placed in the nose or mouth.
In more serious cases, the baby may need to be intubated and placed on a ventilator to deliver higher concentrations of oxygen and assist breathing. The primary goal is to increase oxygen delivery to vital organs throughout the body. In severe cases, inhaled nitric oxide may be used to dilate pulmonary blood vessels, or the baby may require ECMO (extracorporeal membrane oxygenation), a form of heart-lung bypass support used when conventional treatments are not enough
What Can Cause PPHN?
The cause of PPHN is not always known. But we know several things that can cause pulmonary hypertension:
- meconium aspiration syndrome
- amniotic fluid aspiration
- pulmonary hyperplasia
- sepsis
Can Meconicum Aspiration Cause PPHN?
Meconium aspiration can trigger PPHN by causing pneumonia in the lungs, causing vasoconstriction.
When Is PPHN Medical Malpractice?
Not every case of persistent pulmonary hypertension of the newborn is malpractice. PPHN can develop even when doctors do everything right. But some cases are absolutely preventable and these are the cases our lawyers pursue and file.
Most viable PPHN malpractice cases fall into one of three categories:
1. Failure to deliver in time
If fetal monitoring strips show distress, prolonged decelerations, acidosis, or signs of oxygen deprivation, and the medical team delays a C-section, that delay can trigger hypoxia, meconium aspiration, and ultimately PPHN. In many of the largest verdicts, the baby was neurologically intact on arrival but deteriorated during a preventable delay.
2. Failure to recognize and diagnose PPHN quickly
PPHN is a cardiopulmonary emergency. When a newborn is blue, struggling to breathe, or has low oxygen levels that do not improve, doctors must act immediately. That means rapid NICU involvement and prompt echocardiography. Delays in diagnosis can cost critical minutes when the brain is starving for oxygen.
3. Failure to escalate treatment
Once PPHN is suspected, the baby may need aggressive respiratory support, inhaled nitric oxide, blood pressure support, or even ECMO. Some malpractice cases involve hospitals that did not initiate these therapies quickly enough or failed to transfer the baby to a facility capable of providing ECMO. When escalation is delayed, the risk of permanent brain injury rises sharply.
The common thread in strong PPHN cases is oxygen deprivation. If the evidence shows that earlier delivery, faster diagnosis, or quicker respiratory support would more likely than not have prevented hypoxic brain injury or death, the case may be viable.
If, on the other hand, the condition developed suddenly, was promptly recognized, and was aggressively treated according to accepted neonatal standards, it may not be malpractice even if the outcome was tragic.
That is why these cases require careful review of fetal monitoring strips, blood gas results, timing of interventions, NICU records, and transfer decisions. The details matter.
PPHN Settlement Amounts and Jury Payouts
The verdicts and reported settlements summarized below are from medical malpractice cases involving PPHN. The amount of the awards are less important than the stories of what makes for a viable PPN birth injury or wrongful death claim.
-
- Anonymous v. OB/GYN and Hospital (Michigan 2025) $120,654,000.08: A first-time teenage mother with limited prenatal care presented to labor and delivery at 8 p.m. Fetal monitoring strips were Category II, showing mixed variability. Plaintiffs argued the baby was neurologically intact on arrival but that the obstetrician failed to perform an urgent C-section within 30 minutes despite non-reassuring fetal heart tracings and prolonged decelerations. A C-section was ordered at 9:45 p.m., but delivery did not occur until 12:10 a.m., and fetal monitoring was discontinued when the mother was moved to the operating room. Plaintiffs’ PPHN lawsuit contended that the delay caused progressive hypoxia, metabolic acidosis, hypoxic-ischemic brain injury, meconium aspiration syndrome, and persistent pulmonary hypertension of the newborn, which ultimately required ECMO and worsened the brain injury. The defense argued the injuries were due to chronic maternal factors and that any brain damage resulted from a bleed during ECMO. The jury found the physician and four nurses negligent and awarded $120,654,000.08, including future life care costs and projections of lost earning capacity.
- Baby Doe v. AAA Hospital (Michigan 2019) $8 million: A newborn sustained a hypoxic injury after an emergency C-section. This occurred after the labor failed to progress for several hours, even with Pitocin. Following her birth, the NICU staff treated her for PPHN, meconium aspiration syndrome, multi-organ failure, and metabolic acidosis. The girl developed spastic cerebral palsy, cognitive delays, and seizures. She required lifelong assistive care. Her mother alleged that the delay of a C-section caused her permanent injuries. This case settled for $8 million.
- Sodjago v. Pediatrix Medical Group of Georgia (Georgia 2014) $3 million: A post-term baby was born unresponsive, not breathing, and with no heart rate. The hospital staff resuscitated her and raised her blood oxygen levels. The baby suffered from PPHN, which was treated with nitric oxide. Despite undergoing this treatment, she already sustained permanent neurological damage, including cortical blindness, cognitive impairments, and behavioral problems. Her mother alleged that the delay of the nitrous oxide treatment prolonged her PPHN, causing permanent injuries. A jury awarded a $3 million verdict.
- Baby K v Hospital (Florida 2014) $2.9 million: A baby is born with gastroschisis. This is a congenital anomaly where parts of the baby’s organs, including intestines and internal organs, are on the outside rather than inside the baby’s body. Closure surgery is performed to correct the condition, but after the procedure, the baby has trouble breathing. Her oxygen levels slowly deteriorate and she is diagnosed with PPHN. The hospital does not have an extracorporeal membrane oxygenation (ECMO) machine. The baby tragically dies. The parents hire a wrongful death birth injury lawyer and file a lawsuit, alleging the doctors and nurses failed to manage the baby’s PPHN. The family also argued that the child should have transferred to another hospital for an ECMO procedure that would have saved her life. Case settles prior to trial for $2,959,000.
- Sodjago v Pediatrix Medical (Georgia 2013) $3 million: fetal monitoring strips indicate major distress, but a miscommunication between nurses and doctors results in a long delay before an emergency C-section is performed. Baby is not breathing when delivered, but the neonatal resuscitation team restores breathing and heartbeat, but she has PPHN and is not getting enough oxygen. She is eventually given nitric oxide to help open blood vessels to her lungs but prolonged oxygen deprivation leaves her with brain damage, cognitive impairment and partial blindness. Jury awards $3,000,000.
- Plaintiff v Defendant (California 2013) $9.9 million: mother in her late-30s is towards the end of a high-risk pregnancy, further complicated by gestational diabetes, when she goes for a prenatal visit, and doctors find very concerning signs of fetal distress. She is immediately sent to the hospital for delivery, but a series of logistical errors and miscommunications result in an extended delay before a doctor arrives to finally perform an emergency C-section. Baby suffers from hypoxic-ischemic encephalopathy (HIE) injury and persistent pulmonary hypertension of the newborn (PPHN). Baby remains in NICU for 5 weeks and is eventually diagnosed with cerebral palsy with permanent cognitive impairment and developmental delays. Mother sues doctor and hospital for negligent mishandling of labor and delivery and jury awards $9.9 million.
- Ketterman v Capital Women’s Care (Maryland 2009) $1.8 million: This is the most recent PPHN verdict our lawyers could find in Maryland. In this case, the mother in labor attempts pushing for 3 hours, but the baby’s head does not descend into the birth canal and becomes wedged in the mother’s pelvis. Defendant OB/GYN elects to use a vacuum extractor to facilitate delivery. Vacuum pump injures the baby’s head and causes a massive brain bleed, which causes persistent pulmonary hypertension (PPHN). Baby’s PPHN triggers cardiac failure and he dies. Parents sue doctor alleging that his use of the vacuum extractor was negligent and not appropriate given the baby’s position in the pelvis. Defendant claims that the baby’s PPHN developed in utero and was not caused by the vacuum injuries. Jury in Montgomery County finds in favor of plaintiffs and awards $1.8 million in damages.
- Elizarde v Laredo Regional (California 2009) $250,000: 30-year-old mother delivers female baby at only 27-weeks’ gestation. Baby has persistent pulmonary hypertension, which causes her death after 20 hours from cardiopulmonary collapse. Mother sues hospital and doctors, alleging that they were negligent in failing to take a more aggressive approach in the treatment and care of the baby after birth. Specifically, they allege that the baby should have been immediately intubated. Defendants insist that more aggressive intervention was not mandated under the circumstances. The case settles for $250,000
PPHN Medical Literature
In a birth injury lawsuit involving PPHN, experts and attorneys on both sides will use medical literature to make their case to the jury. These are some of the articles you can expect to see used in litigation.
Hire a PPHN Birth Injury Lawyer
The birth injury attorneys at Miller & Zois can help you investigate your PPHN case and pursue any potential claims for medical malpractice. Call us for a free consultation at 800-553-8082 or submit an online contact form.