






A lawyer handling a birth injury malpractice lawsuit needs to read fetal heart strips like an obstetrician. Electronic fetal monitoring and the interpretation and reaction to fetal heart strips are critical focal points in almost every birth injury lawsuit.
Often, birth injury lawsuits involve the failure to identify and respond when the fetus shows recurrent late decelerations on the fetal heart monitor.
The purpose of this page is to help lawyers and parents better understand how to read recurrent late decelerations on fetal heart monitor strips and understand their potential significance when evaluating what went wrong during the delivery process.
-
RECURRENT LATE DECELERATIONS TABLE OF CONTENTS
Category III Fetal Heart Strips: Recurrent Late Decelerations
Categories of Fetal Heart Tracing
What Is a Category 3 Fetal Heart Tracing?
Category 3: Minimal Variability with Recurrent Late Decelerations
What Do Late Decelerations Look Like?
Why Are Late Decelerations Dangerous?
What Conditions Cause Late Decelerations?
What Does a Category 3 Strip With Minimal Variability and Recurrent Late Decelerations Look Like?
Can Recurrent Late Decelerations Be Corrected?
Doctors and Nurses Have to Stay on Top of the Baby’s Condition
What Are Late Decelerations on a Fetal Monitor?
Late decelerations refer to a specific pattern on a fetal heart monitor that typically signals uteroplacental insufficiency. So the placenta is failing to deliver adequate oxygen to the fetus during labor. The fetal heart rate pattern can be a marker of fetal cardiac and central nervous system responses to significant changes in blood gases, blood pressure, and acid-base status.
This is not merely a clinical footnote to keep in the back of your head. It is the baby telling us that it may be in distress. When these decelerations occur repeatedly and are accompanied by minimal variability in heart rate, the situation demands urgent evaluation.
Definition of Late Deceleration
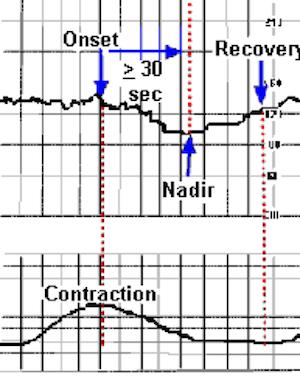
A late deceleration is a gradual slowing of the fetal heart rate that begins after a uterine contraction has started and returns to baseline only after the contraction has ended. This timing is what defines the pattern as “late,” as opposed to variable decelerations, which may appear abruptly and are not always tied to contractions. A variable deceleration is defined as an abrupt decrease in fetal heart rate of at least 15 beats per minute, lasting at least 15 seconds but less than 2 minutes, measured from the onset of the drop to the return to baseline.
When this pattern shows up with at least half of the contractions, it is classified as recurrent late decelerations. This designation often correlates with fetal hypoxia and a deteriorating intrauterine environment which means that action needs to be taken.
How to Recognize Late Decelerations on a Strip
On an electronic fetal monitoring strip, late decels appear as smooth, shallow U-shaped dips in the fetal heart rate. They do not start until after the contraction begins, and they do not reach their lowest point until after the contraction has peaked. They then return to baseline only once the contraction is fully resolved. These decelerations are not abrupt. They are gradual and deliberate in appearance. The presence of minimal beat-to-beat variability alongside these dips is particularly dangerous. It moves the tracing into the clinically defined Category III, a high-risk classification that typically warrants immediate action.
Why Recurrent Late Decelerations Matter
Recurrent late decelerations are not merely a diagnostic observation. They are a call to act. Their presence often signifies that the fetus is experiencing hypoxia. If not addressed promptly, these decelerations can lead to bradycardia and may ultimately result in lasting injury, including cerebral palsy or other neurological damage. Clinicians are expected to intervene—whether by repositioning the mother, discontinuing uterotonic agents like Pitocin, or moving quickly toward surgical delivery.
For birth injury lawyers, recurrent late decelerations often become a central issue in malpractice litigation. A strip that shows repeated late decelerations without an appropriate response provides a powerful window into what went wrong during labor. These cases do not usually hinge on complex theories of causation. They hinge on the failure to respond to unmistakable signs of fetal distress, which are clearly recorded in real-time.
Categories of Fetal Heart Tracing
Before we read the tracings, it is important to understand the general categories of strips. For a description of these fetal heart tracing categories, please read our summary on Categories of Fetal Heart Tracings.
What Is a Category 3 Fetal Heart Tracing?
A Category 3 fetal heart tracing is predictive of an abnormal fetal acid-base status, meaning that the fetus is not getting enough oxygen. Category 3 fetal heart tracings usually require immediate action and prompt delivery via cesarean section. Category III tracings had the highest risks for umbilical artery pH <7.0 and hypoxic ischemic encephalopathy, while the risks of both were lower and not significantly different for category I and II tracings.
Clinical Response to Recurrent Late Decelerations
- Moderate variability: Consider reversible causes (position, fluids, reduce Pitocin).
- Minimal/absent variability: Category III – requires urgent evaluation.
Failure to act on this progression is a common cause of birth injury malpractice lawsuits, especially in cases involving cerebral palsy or stillbirth.
Category 3: Minimal Variability with Recurrent Late Decelerations
There are many different types of Category 3 fetal heart tracing. This page is focused on minimal variability with recurrent late decelerations (late decels) during labor.
What Do Late Decelerations Look Like?
Unlike a variable deceleration, which appears as an abrupt decrease in fetal heart rate and may not be associated with a contraction, a late deceleration begins after a uterine contraction has started. The fetal heart rate does not return to baseline until well after the contraction has ended.
Visually, late decelerations look very different than variable decelerations. Unlike variable decelerations that look like an upside-down mountain, late decelerations appear as a “U” or “W” shape. They are less abrupt and usually not as pointed. The return to a baseline heart rate is gradual over a period of time. You can see the difference between a late deceleration and a variable deceleration below.
Variable Deceleration:
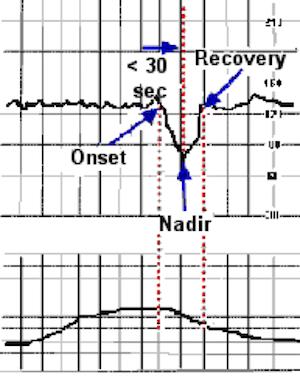
Late Deceleration:
Why Are Late Decelerations Dangerous?
Late decelerations are dangerous because they are evidence of uteroplacental insufficiency. The placenta is the fetus’s lifeline from the mother. Vital blood and oxygen flow from the mother’s uterus to the placenta and into the umbilical cord to the fetus.
If there is a disruption in the transfer of blood, nutrients, and oxygen from the uterus to the placenta, the fetus will begin to suffer.
So when late decelerations recur with more than half of contractions, and are paired with reduced variability, they are classified as Category III traces, indicating high risk for fetal acidemia and often prompting immediate intervention.
What Causes Late Decelerations?
There are many dangerous conditions that can cause late decelerations. A few common ones are as follows:
- Placental abruption
- Maternal diabetes
- Gestational hypertension
- Preeclampsia
- Maternal anemia
- Maternal sepsis
- Post-term pregnancy
- Hyper-stimulated uterus
Whenever late decelerations occur, it is crucial for nurses and physicians to document them in the medical record and to monitor the patient closely. If late deceleration begins to occur more frequently, or if they are associated with other fetal heart strip abnormalities, such as minimal variability, the physician may need to perform an emergency cesarean section.
Variable decelerations can be subtle, but the key is how the heart rate is trending. The risk of serious injury or death is high when doctors and nurses ignore the warning or fail to recognize that periods of minimal variability accompanied by recurrent late decelerations are indicative of abnormal fetal acid-base status and hypoxia.
What Does A Category 3 Strip With Minimal Variability and Recurrent Late Decelerations Look Like?
The top portion of the fetal heart strip represents the fetal heart rate, while the bottom portion represents the mother’s uterine contractions.
As you can see from the tracing, there are late decelerations occurring with every contraction. The decelerations do not begin until after the contraction has started. There is a gradual dip in the fetal heart rate with a return to baseline heart rate after the contraction has stopped. There is minimal beat-to-beat variability between contractions. The baseline heart rate measured over 10 minutes is 130 beats per minute.
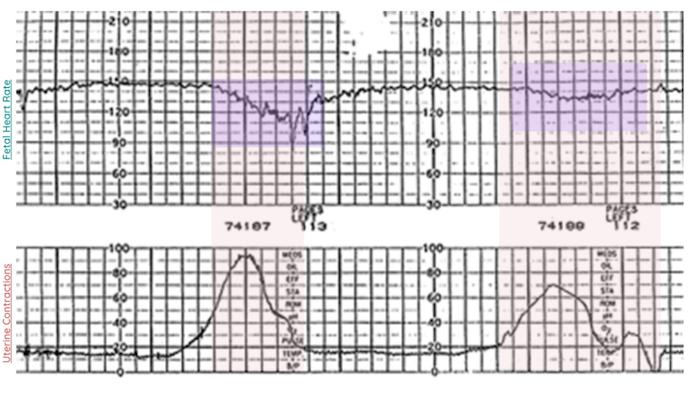
One thing that is worth noting is that not all late decelerations are created equal. In the example above, a prominent late deceleration occurs with the first contraction, whereas a shallow, subtle late deceleration occurs with the second contraction.
Unlike variable decelerations, where the depth of the variable deceleration may signal a potential problem, all late decelerations should put doctors on notice of the likely need for immediate delivery. Recurrent late decelerations, especially when paired with minimal or absent variability, put the team on notice that urgent escalation and possible expedited delivery may be necessary.
Even if the late decelerations have different depths, they must be considered dangerous. If they are recurring, even with moderate variability in between, it is incumbent upon the nurses and physicians to assess the fetus’s condition.
Can Recurrent Late Decelerations Be Corrected?
Sometimes, but it depends. Recurrent late decelerations with moderate variability in between may be caused by excessive uterine contractions or low blood pressure. Sometimes, these conditions can be corrected by reducing the contraction or increasing the blood pressure. This can be done by reducing the Pitocin, providing intravenous fluids, or changing maternal position.
That said, certain medical conditions, such as diabetes, high blood pressure, and intrauterine growth restriction, may be associated with measures to improve blood flow and oxygenation that are not successful. If the lack of oxygen continues, the fetus may develop acidosis and suffer injury.
If the fetus is deprived of enough oxygen, the child might go from having late decelerations to no decelerations or bradycardia (low heart rate below 60 beats per minute). Doctors should not wait until this kind of emergency occurs.
Doctors and Nurses Have to Stay on Top of the Baby’s Condition
Ultimately, it is the responsibility of nurses and physicians to read and interpret fetal heart tracings, not only by interpreting the tracing but also by considering it in the context of the patient’s condition.
A fetal heart strip with moderate variability and recurrent late decelerations (a Category 2 strip) could quickly become a Category Three strip with minimal variability and recurrent late decelerations, requiring an emergency cesarean section.
Most of the time, these fetal heart strips do not show miraculous improvement. For this reason, it is also vital for a physician to consider the mother’s condition. Category 3 fetal heart tracings often occur with diabetic mothers, high-risk pregnancies, twin pregnancies, growth restriction, or hypertension.
If a patient has one of these conditions, it must be assumed that it is the cause of the problem. A patient developing such a pattern in this context may need to be considered for delivery before the condition worsens. There simply is nothing to be gained by waiting for something bad to happen.
Medical Malpractice and Late Decelerations
When late decelerations appear on a fetal heart monitor, particularly when they recur and are accompanied by minimal variability, they are not subtle. The baby is telling you loud and clear that there is fear of fetal compromise, recorded in real time and demanding clinical attention. The failure to recognize these signs or act on them promptly often forms the basis of a birth injury lawsuit.
The standard of care requires obstetric teams to interpret fetal monitoring patterns accurately and to intervene when the tracing moves from Category I or II into Category III. That intervention might mean repositioning the mother to improve blood flow, halting uterotonic medications like oxytocin, or preparing for an urgent cesarean delivery. When providers hesitate—when they watch late decelerations mount without escalating care—the window for preventing irreversible harm narrows with every contraction.
In many birth injury lawsuits, late decelerations become the crux of the case. They offer a timeline of what the baby was experiencing—and what the providers did or failed to do in response. If your child suffered injury due to delayed recognition of fetal distress, or if the medical team dismissed warning signs until it was too late, you may have grounds for a malpractice claim. These are not speculative cases—they are built on objective evidence and a clearly defined clinical standard. And they are cases that deserve to be pursued.
Getting Help from a Birth Injury Lawyer
If you have a birth injury claim and you are not sure if you have a case, or if you are a lawyer looking for help handling your client’s birth injury, call us today. You can reach our birth injury lawyers at 800-553-8082 or you can get a free consultation online.