






Our law firm handles malpractice lawsuits for birth injuries from shoulder dystocia. Our shoulder dystocia lawyers are based in Maryland. But our attorneys handle serious injury and wrongful death birth injury lawsuits throughout the country. We often partner with the best handpicked attorneys in other jurisdictions like Georgia, Illinois, Pennsylvania, and others states. The focus is to maximize the shoulder dystocia settlement amount or jury payout for you while you pay the attorneys’ fees for just one lawyer. And you only pay a fee if our shoulder dystocia lawyers obtain a recovery for you.
Understanding Shoulder Dystocia
Shoulder dystocia is an obstetrical complication that occurs in 30,000 deliveries in the U.S. each year. Shoulder dystocia and brachial plexus injury occur in .5% to 1.5% (or more) of all births.
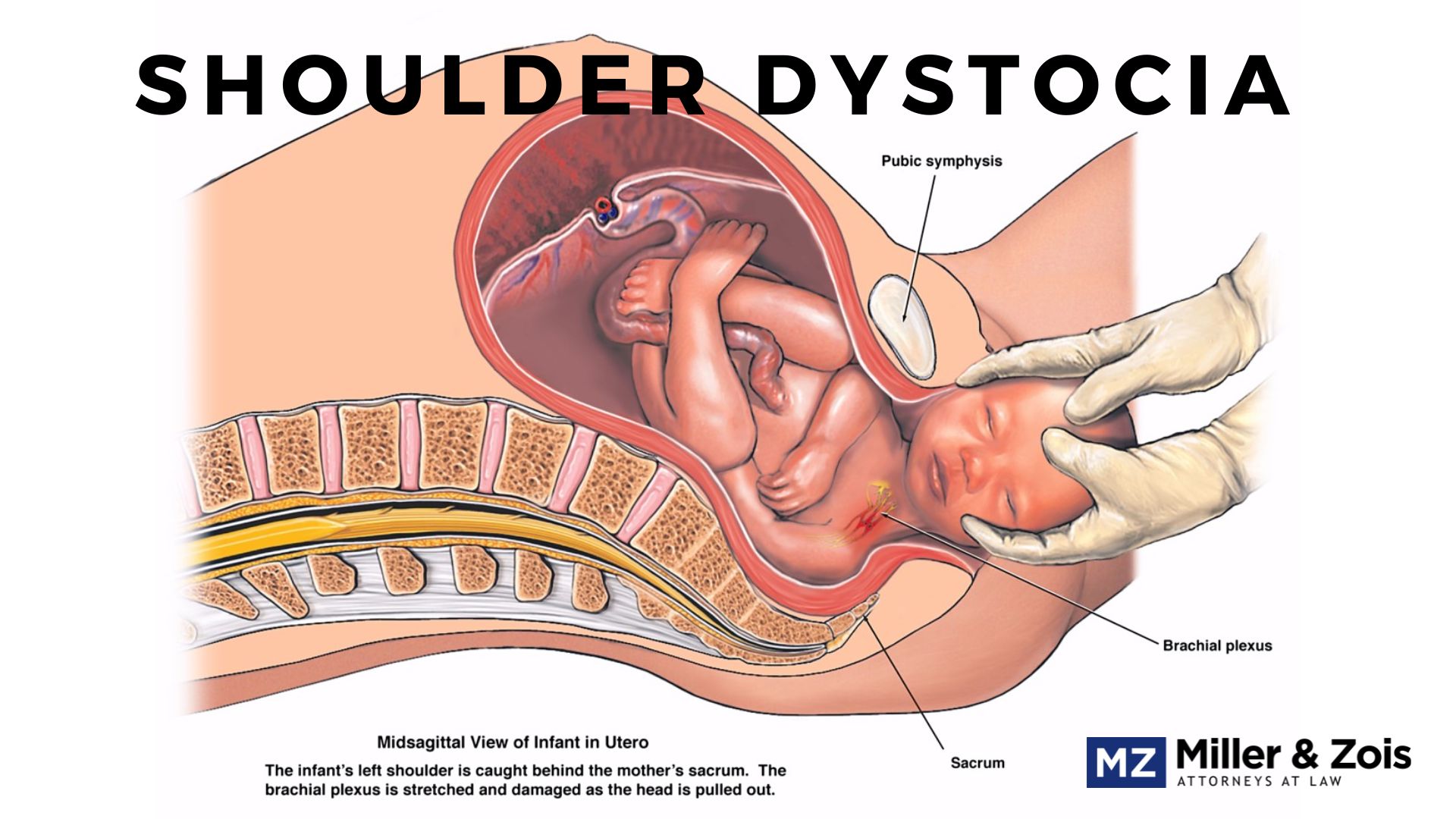
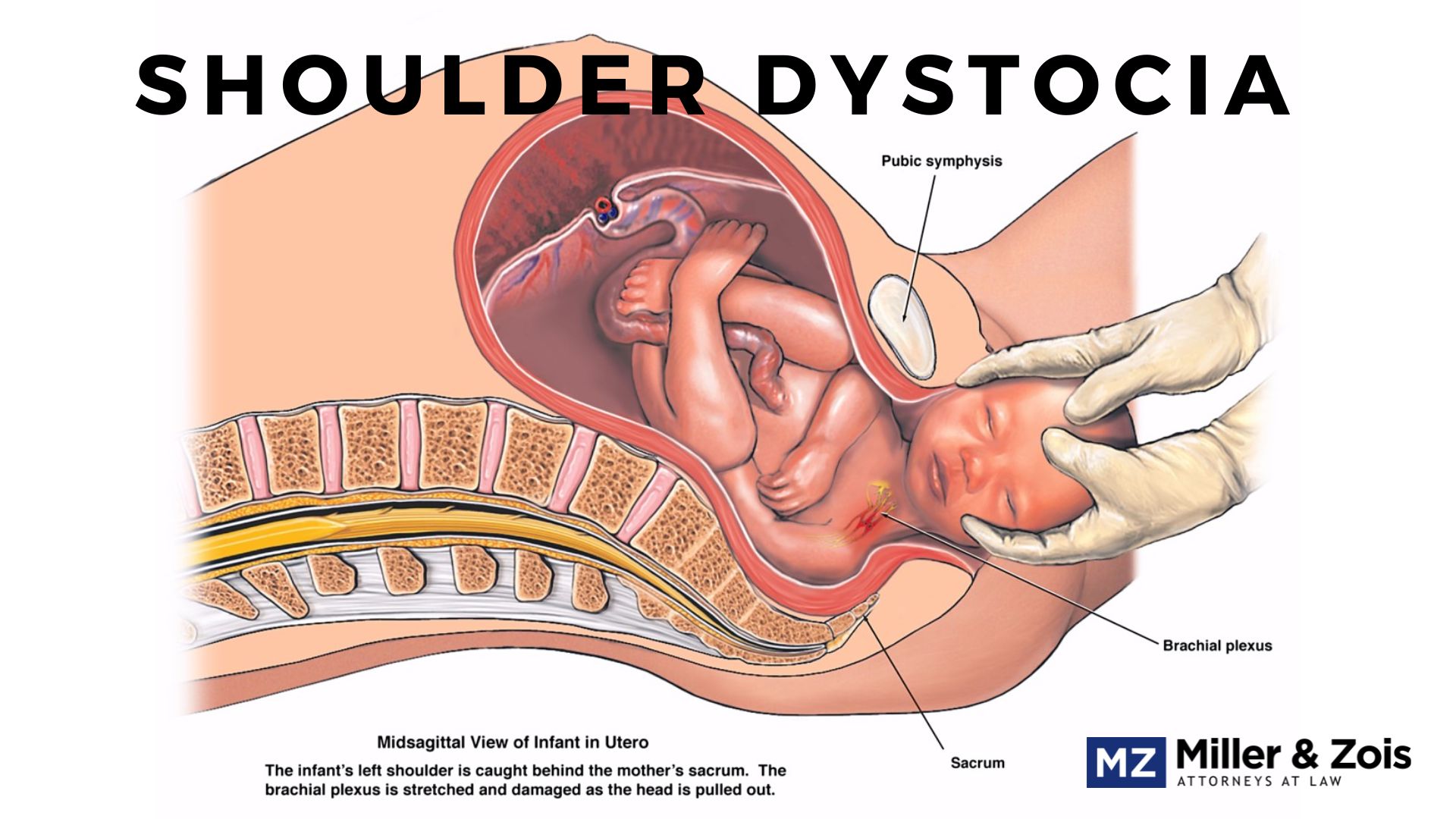
Shoulder dystocia stems from complications during childbirth where the child’s head can clear the pubic symphysis, but the shoulders require additional medical maneuvers to be correctly delivered. In a shoulder dystocia case, typically one shoulder of the baby becomes trapped behind the mother’s pelvis during delivery.
So in a normal delivery, the head delivers and there is a progression, in the same contraction or with the next contraction, and within a minute or two, the rest of the baby is delivered. In a shoulder dystocia case, the head delivers and the rest of the baby does not. The obstetrician has to manage this problem.
Are all shoulder dystocia cases legitimate malpractice claims? No. But most doctors that have taken a serious look at this issue agree that a significant number of these shoulder dystocia lawsuits are meritorious.
What happens? The medical literature tells us that birth assistive techniques used in the presence of shoulder dystocia that either pull on the infant’s head (forceps, vacuum extraction, manual traction, and fundal pressure are both associated with Erb’s Palsy and other brachial plexus injuries.
How Medical Malpractice Can Cause Shoulder Dystocia
Shoulder dystocia has been called the OBs Achilles’ heel because mistakes made throughout the pregnancy come home to roost during childbirth.
For example, a mistake made during prenatal testing or failing to get a proper history of the mother can be revealed when shoulder dystocia presents itself during childbirth. So it is not just a question of technique and decision-making during delivery.
That said, many mistakes are made during the birthing process. Once the obstetricians realize that a baby’s shoulder is stuck on the pelvic bone, the OB/GYN has a limited window of opportunity to perform one or more of the well-known maneuvers to free the shoulder and deliver the baby safely.
Techniques to Resolve Shoulder Dystocia
The four techniques obstetricians use when the shoulder is stuck during delivery:
- McRobert’s maneuver
- Suprapubic pressure
- Woods screw maneuver
- Delivery of the posterior arm
McRoberts
The “McRobert’s maneuver” is usually the starting point technique to resolve shoulder dystocia. The goal is to dislodge the fetus’s shoulder without causing injury. (This is a good image that shows this technique.)
Using McRoberts, the mother’s legs are taken out of the stirrups. The nurses push the mother’s thighs up and hyperflex her knees back to her chest. This moves move tailbone forward and the pubic bone back. The result of the McRoberts maneuver typically gets the baby’s shoulder to slip out more easily because you have increased the diameter of the pelvis.
So the McRoberts’ maneuver reduces the overall extraction force that is needed for delivery and significantly reduces the contact force behind the symphysis pubis.
Suprapubic Pressure
If McRoberts fails, the next technique is usually suprapubic pressure. This is rotating the baby’s shoulder out from under the public bone. You take your fist and find the shoulder with an open hand or fist above the symphysis pubis. That pressure is placed to the left, right, or straight down to rotate the shoulder.
The goal is to push the baby’s shoulder out from the obstructing public bone. This procedure will work within 30 seconds or it is time to move to plan C.
Some birth injury malpractice cases are the result of doctors staying with this technique too long or panicking and using the incorrect hand placement, causing uterine rupture or pushing the shoulder even further behind the pubic bone.
Woods Screw Maneuver
The Woods’ screw maneuver puts pressure on the posterior shoulder like you would use a corkscrew to release the opposite impacted anterior shoulder. The hope is it turns the anterior shoulder to the posterior and vice versa. There is also a geometry to this technique.
Putting pressure on the posterior shoulder will flex the shoulders across the chest. This decreases the distance between the shoulders. This, in turn, decreases what can fit through the pelvis. Anyone who has moved a large object through a door frame understands this idea.
Delivery of the Posterior Arm
This is another geometry-type move to knock a few centimeters off the diameter. The doctor or nurse places her hand in the vagina, finds the baby’s hand, and tries to move the arm in a sweeping motion towards the center of the body.
Stay Off the Head
The key point is that none of these maneuvers requires touching the infant’s head. But, regrettably, doctors – often some very good doctors – panic when they see the head of the baby is delivered but then retracts against the perineum (the first sign of the problem).
What happens is the doctor applies excessive traction laterally to the neck – pushing the head toward either shoulder – that mistake can cause shoulder dystocia and other complications.
The physician fears that if the shoulder is not quickly dislodged, the baby cannot breathe, and there is a risk of death by suffocation. Some doctors panic when the baby cannot be successfully delivered. It has to be terrifying.
But obstetricians are trained to handle this panic and to employ certain medical techniques that must be employed to manage the labor and reduce the risk of shoulder dystocia. If they do not employ these medical techniques and try to laterally force the baby out, or otherwise take steps outside of the standard of care, the doctors can cause harm to the baby and mother that leads the family to contact a medical malpractice lawyer about a potential malpractice lawsuit.
Our birth injury lawyers sometimes sue the nurse as well. The nurse often applies fundal pressure to the infant’s shoulder against the pubic bone which will further compound the problem.
So if a nurse deviated from the standard of care by applying fundal pressure, th
ere is wisdom in naming the nurse the facility or hospital as defendants in any lawsuit as opposed to just the doctor. (This can also impact the amount of insurance coverage in a birth injury case because the hospital has a large policy and significant assets.)
What Will the Doctors’ Medical Malpractice Lawyers Argue?
The arguments that defendants’ medical malpractice lawyers in Maryland make in shoulder dystocia cases vary from case to case. One thing is for sure: the doctors will paper the file with excuses.
Not all shoulder dystocia cases are caused by medical malpractice. But in meritorious shoulder dystocia malpractice lawsuits, these are some of the arguments doctors’ medical malpractice lawyers make:
Doctor’s Argument: Even if the delivering doctor applied excessive force, the doctor did so because there was no alternative.
Plaintiff’s Response: Because lateral traction is the only known cause of Erb’s palsy in head-first vaginal deliveries, it is a breach of the standard of care because the procedure cannot free the shoulder anyway.
Doctor’s Argument: The baby was delivered without incident. The baby’s complications must have occurred in utero. In support, these lawyers point to the medical literature supporting this proposition.
Plaintiff’s Response: The baby’s malpractice attorney and their medical expert can counter these articles by pointing out they are not case reports by treating obstetricians. Instead, the articles review medical records of mothers who have had infants who had shoulder dystocia. If the doctor does not admit to how the delivery occurred, the articles become utterly useless.
Doctor’s Argument: The shoulder dystocia occurred because the fetus was too big.
Plaintiff’s Response: Shoulder dystocia is foreseeable because birth weights can be predicted. Typically, some signs forebode a large baby such as the mother previously having large children, gestational diabetes, or maternal obesity. A sonogram can also assist in predicting birth weight. If this information leads the doctor to believe that the baby is going to be excessively large, preventive steps should be taken (such as a cesarean section). (A baby weighing more than 8.13 ounces at birth has a five times greater risk of suffering shoulder dystocia during birth than a child weighing less.)
Cephalopelvic Disproportion Malpractice
Cephalopelvic disproportion (CPD) is another birth injury that is similar to shoulder dystocia. With cephalopelvic disproportion, the difference between the size of the baby’s head or the body and the size of this birth canal makes a vaginal birth just too risky. This can be either because the baby is too big for the birth canal or the birth canal is too small for the baby.
Either way, the failure to perform a cesarean section in the face of this problem can be medical malpractice. An obstetrician has a duty to monitor that pelvis and the fetus through the various stages of pregnancy and if cephalopelvic disproportion becomes a concern, the doctor has an obligation to take the necessary steps to mitigate the risk to the mother and child.
Settlement Compensation Payouts in Shoulder Dystocia Cases
The settlement amounts in a shoulder dystocia malpractice case depend on the type of birth injury involved. The majority of shoulder dystocia cases involve brachial plexus nerve injuries resulting in Erb’s palsy.
In some instances, however, mismanagement of shoulder dystocia can result in oxygen deprivation and cause serious brain injuries. Listed below are a number of recent shoulder dystocia settlements and verdicts that involve allegations of negligent handling of shoulder dystocia resulting in Erb’s palsy or some other type of nerve injury.
- K.L. v Mercy Clinic (Missouri 2024) $2.4 million: The delivery team encountered shoulder dystocia after the infant’s head was delivered. The plaintiff reportedly sustained a brachial plexus injury to his right upper extremity with damage to the C5-C7 spinal nerves and ptosis to the right eye, diagnosed as Horner’s Syndrome. According to the plaintiff, the defendant OBGYN utilized excessive force in the vaginal delivery which resulted in the injuries.
- W.M. v Dautrive (Louisiana 2022) $15.0 million: The baby sustained a brachial plexus injury to his left shoulder and C5-C7 spinal nerve damage, and was left with permanent, lifelong dysfunction and disfigurement of his left shoulder and arm. The lawsuits alleged that the defendant failed to realize that the mother, as a diabetic first time mother, was at an increased risk of encountering shoulder dystocia during labor and failed to have a plan in place if same occurred; used excessive traction and manipulation, attempting a dangerous midforceps assisted delivery of the infant; failed to utilize appropriate maneuvers to dislodge the shoulder from the birth canal.
- Plaintiff v. Defendant (Virginia 2021) $900,000: The plaintiff was hospitalized at 39 weeks for induction due to an anticipated large fetal weight, informed by gestational diabetes and the birth weights of her previous children. During the delivery, a potential shoulder dystocia was identified when the baby’s head emerged. The attending obstetrician applied downward traction, despite later asserting the use of only gentle force. The baby’s shoulder remained lodged against the mother’s pubic bone, and it took several maneuvers, including a rotational technique, to complete the delivery. Immediately post-delivery, an injury to the baby’s left arm became evident. Subsequent evaluations showed permanent nerve injuries at the C5-C8 levels, with significant neuromas and avulsions that have adversely affected the child’s daily life and mobility. The defendant’s shoulder dystocia lawyer gave the class defense to excessive traction lawsuits: shoulder dystocia in unpredictable and natural forces caused it. Plaintiffs’ expert witnesses pushed back on the maternal forces of labor argument, emphasizing standard delivery protocols and said excessive force by the obstetrician caused the injuries. The parties ultimately agreed to a $900,000 settlement.
- Olukanni v. Ghazi (Pennsylvania 2020) $1.15 million: A newborn was delivered with the assistance of a vacuum. A vacuum extraction is designed to facilitate labor by delivering the head. A vacuum extraction on a woman who is delivering that large baby will increase the risk of shoulder dystocia. He sustained sublegal hemorrhaging and hypoxic-ischemic encephalopathy. The boy died hours later. His parents alleged negligence against the OB/GYN. They claimed he failed to appreciate fetal bradycardia signs, properly address shoulder dystocia, perform an emergency C-section, and timely resuscitate their son. This case settled for $1.15 million.
- S.G., Pro Ami v. Garden City Obstetrics and Gynecology, P.C. (New York 2020) $3.05 million: A newborn suffered Erb’s palsy, Klumpke’s palsy, and nerve root avulsion. She was left with cosmetic deformities. The girl’s mother alleged negligence against the OB/GYN practice. She claimed its physicians improperly addressed shoulder dystocia, negligently performed a vacuum-assisted delivery, used excessive Pitocin doses, failed to appreciate cephalopelvic disproportion, and failed to perform an emergency C-section. This case settled for $3.05 million.
- V. S-D., Pro Ami v. Hahnemann University Hospital (Pennsylvania 2020) $850,000. A baby girl suffered brachial plexus neuropathy, Erb’s palsy, and a left humerus fracture at birth. She was left with permanent left shoulder and arm disabilities. The girl’s adoptive parents alleged negligence against the hospital. They claimed its staff failed to appreciate shoulder dystocia, counsel the birth mother on a vaginal delivery’s risks, appropriately administer Pitocin, offer a C-section, and perform an emergency C-section. This case settled for $850,000.
- Unnamed Plaintiff v. Unnamed Defendant (Virginia 2020) $615,000: A mother went to a hospital’s labor and delivery department to deliver her first child. During labor, her baby had an abnormal fetal heart rate. The OB and the hospital staff did not offer the option of a C-section. They encountered shoulder dystocia during the vaginal delivery. The obstetrician then attempted a Zavanelli maneuver and a C-section. These attempts were unsuccessful. The baby was delivered but lived only for 42 minutes. The mother’s experts planned to testify that the baby would have survived if they were delivered earlier. This case settled for $615,000.
- Unnamed Plaintiff v. Unnamed Defendant (Virginia 2019) $2 million: A baby experienced hypoxic-ischemic encephalopathy because of a delayed vacuum-assisted delivery. The initial fetal heart strips, that followed labor induction, showed reassuring results. However, labor failed to progress. Hospital staff administered Cytotec and Pitocin. The fetal heart strip results eventually revealed abnormalities. The mother’s uterine contraction patterns showed persistent tachysystole. Nursing staff attempted several resuscitative measures, which failed to resolve the fetal heart rate. Near the end of labor, the fetal heart rate showed a hypoxic risk. The obstetrician attempted to manually rotate the fetus. He then used a vacuum extractor and discovered shoulder dystocia. The baby was born not breathing, cyanotic, and lacked muscle tone and reflex. He developed seizures after being resuscitated. Doctors diagnosed him with hypoxic-ischemic encephalopathy, spast
ic cerebral palsy, cortical blindness, cystic encephalomalacia, microcephaly, and hemiparesis. This case settled for $2,000,000 before trial. - Perez v. Hu (Indiana 2018) $2 million: A mother attempted to give birth to a macrosomic baby. She had a medical history of obesity, gestational diabetes, and previously given birth to a baby weighing over ten pounds. The mother was admitted to the hospital, where the obstetrician prescribed Pitocin to induce labor. The obstetrician delivered the baby’s head but discovered shoulder dystocia. He applied the McRoberts maneuver to complete the delivery. However, this was unsuccessful. The obstetrician then applied traction, and the baby was born shortly after. The baby was revealed to have suffered a brachial plexus injury, a permanent neurologic injury, and a subdural hematoma. His left arm became permanently paralyzed. The mother sued the obstetrician, alleging his failure to get informed consent for a vaginal delivery and to discuss a C-section option. The jury awarded $2,000,000, which the court reduced to a statutory maximum of $1,250,000.
- A.H. v. Gonzalez (Virginia 2018) $2.3 million: Inova Fairfax Hospital admitted a woman who was to deliver her child. The prenatal course and labor appeared normal. However, the obstetrician discovered shoulder dystocia after delivering the head. He attempted several maneuvers, but they were unsuccessful. The obstetrician then applied traction to the baby’s head multiple times. He was successful in releasing the baby’s shoulder and delivering the baby after the second round of maneuvers. The baby suffered a non-functioning right arm that lacked strength. His mother sued the obstetrician for applying excessive traction that caused her baby’s permanent arm injuries. The jury awarded a $2,320,335 verdict.
- Unnamed Plaintiff v. Unnamed Defendant (Virginia 2018) $1.1 million: A mother sued an obstetrician, alleging delivery mismanagement. She alleged that the inexperienced obstetrician wrongly attempted maneuvers to release the baby’s shoulder after he discovered shoulder dystocia. The baby suffered a brachial plexus injury and nerve avulsion. They underwent surgeries to repair their injuries, which proved to be unsuccessful. The case settled for $1,100,000.
- Samuelson v. Allina Health System (Minnesota 2018) $8.9 million: A woman sued a midwife and a hospital for mismanaging the delivery of her second child. She told the midwife her concerns that the baby was macrosomic. The midwife reassured her that the baby would weigh less than six pounds. The mother alleged that she was never given the option of undergoing a C-section. During labor, shoulder dystocia occurred. The midwife attempted maneuvers that caused his cervical nerves to avulse. She called for help, and the responding physician performed an episiotomy. The baby was delivered shortly after, weighing ten pounds. He suffered nerve avulsions to his neck, a humerus fracture, and Horner syndrome. The jury found the midwife negligent. The jury awarded the mother $8,986,957 in damages.
- Botello v. McLaughlin (New Mexico 2018) $73.1 million: A diabetic woman gave birth to a baby who suffered a brachial plexus injury and brain damage. During labor, the obstetrician encountered shoulder dystocia. He used a vacuum-extraction device to pull the baby out of the birth canal. The baby weighed over 11 pounds. He suffered a brachial plexus injury to his right shoulder and arm. He also suffered brain damage caused by oxygen deprivation as his head was stuck in the birth canal for 10 minutes. His parents hired a shoulder dystocia lawyer who claimed that he could not move his right hand and required lifelong assistance. The mother also suffered lacerations to her vagina and rectum because of the obstetrician’s actions. She experienced emotional trauma. The jury awarded $73,100,000 in damages.
- Henry v Harris (Ohio 2018) $2.75 million: The newborn suffered permanent brachial plexus injury during shoulder dystocia when defendant improperly used extreme downward traction and positioned the infant’s head at a lateral angle during delivery. Defendant was allegedly negligent in continuing with vacuum extraction instead of ordering an emergency C-section.
- Oliva v United States (Michigan 2017) $450,000: Nurse midwife at the hospital allegedly failed to recognize shoulder dystocia during delivery, applied excessive traction on the baby’s head, and failed to perform appropriate maneuvers. The baby was diagnosed with Erb’s palsy and permanent impairment of the left arm. Parties entered into a structured settlement agreement for $450,000.
- McAllister v Lancaster Hosp. (Pennsylvania 2017) $1 million: The plaintiffs alleged that defendants (OB/GYN and Hospital) involved in the delivery of the infant male failed to appreciate the risks involved in the pregnancy and failed to properly manage shoulder dystocia resulting in a brachial plexus injury and loss of the use of the right arm. The defendants denied all allegations of negligence and argued that they were forced to act quickly because the umbilical cord became wrapped around the baby’s neck. Case settled prior to trial for $1,000,000.
- EP v EVMS Medical Group (Virginia 2017) $1.15 million: Baby reportedly suffered brachial plexus injury during delivery resulting in Erb’s palsy and leaving him with limited functionality in his arm. A birth injury lawsuit was filed alleging that the defendant OB/GYN failed to properly anticipate shoulder dystocia and perform a preemptive C-section and then failed to effectively manage shoulder dystocia during delivery. The defendant was insistent that she did not cause the injury and only used gentle traction to facilitate delivery, but this birth injury lawsuit eventually settled for $1.15 million.
- Georges v OB/GYN Services (Connecticut 2016) $4.2 million: Baby suffered brachial plexus injury during delivery and was diagnosed with Erb’s palsy. The midwife was allegedly negligent in failing to timely diagnose shoulder dystocia in utero. When shoulder dystocia became apparent during delivery, the midwife allegedly used excessive lateral traction causing the nerve injury. Erb’s palsy left the baby with permanently impaired movement of her arm and shoulder. After a 6-day trial, the jury awarded the plaintiff $4.2 million in damages.
Contacting a Medical Malpractice Lawyer in Maryland
Shoulder dystocia followed by permanent brachial plexus injury or mental impairment is one of the leading causes of health care mistake lawsuits against health care providers in Maryland. The baby’s mother can also suffer injuries such as uterine rupture or rectovaginal fistulas.
If you believe that you or your child has been injured as the result of a physician’s negligence, call Miller & Zois at 800-553-8082 or click here for a free online consultation.
Plaintiffs’ Shoulder Dystocia Medical Literature
Below are some medical journal articles and ACOG guidelines birth injury lawyers may want to show to their experts:
- Gurewitsch All
en ED, Allen RH, et. al: Improving shoulder dystocia management and outcomes with a targeted quality assurance program. Am J Perinatol. 2017;34:1088-96. - Am. College of OB/GYN, Practice Bulletin, Gestational Diabetes Mellitus, Number 180, 2017
- Crofts JF, et al. Prevention of brachial plexus injury-12 years of shoulder dystocia training: An interrupted time-series study. Brit J Obstet Gynaec. 2016;123(1):111-8.
- Tamura A, et. al: Strain rate effect on the tensile behavior of fiber bundles isolated from a nerve root. Proceedings of sustainable research and innovation; 2015 May 5 (pp. 80-85)
- Gonik B, et. al: Effect of clinician-applied maneuvers on fetal brachial plexus strain during shoulder dystocia delivery. Am Coll Obstet Gynecol. 2010;189(6): S200.
- Allen RH, et. al: Comparing mechanical fetal response during descent, crowning, and restitution among deliveries with and without shoulder dystocia. Am J Obstet Gynecol. 2007;196(6):539.e5.
- Allen RH. On the mechanical aspects of shoulder dystocia and birth injury. Clin Obstet Gynecol. 2007;50:607-23.
What Are the Maternal Complications Associated with Shoulder Dystocia?
Shoulder dystocia can lead to serious complications for the mother as well as the baby. The most common maternal health complication associated with shoulder dystocia is postpartum hemorrhage. Additional complications or maternal injuries include cervical or vaginal lacerations and damage to the rectum and bladder.
What Is Shoulder Dystocia and Compressed Umbilical Cord?
Shoulder dystocia can often lead to problems with the umbilical cord such as cord compression. Umbilical cord compression occurs during labor and delivery when the umbilical cord gets compressed or pinched, disrupting the supply of oxygen to the baby. In some cases of shoulder dystocia, the umbilical cord can get compressed against the mother’s pelvic bone by the baby’s stuck shoulder. This type of compression can be very dangerous and lead to brain damage.
What Does a Compressed Umbilical Cord Mean?
A compressed umbilical cord means that the umbilical cord connecting mother to baby has become pinched or constricted inside the womb. This usually occurs when the baby’s body pushes the cord up against the birth canal or mother’s pelvis. Cord compression can be very dangerous because it can restrict the supply of maternal oxygen to the baby during delivery.
How Dangerous Is Shoulder Dystocia?
Shoulder dystocia is one of the most dangerous obstetric complications that can occur during childbirth. When this complication occurs it is considered an obstetric emergency and if not managed and handled immediately it can lead to serious birth injuries such as cerebral palsy, or HIE.
Can a Baby Die from Shoulder Dystocia?
Although very rare, a baby can potentially die from shoulder dystocia if it is not properly managed in the delivery room. If doctors are not able to free the baby’s shoulder and delivery quickly, oxygen deprivation can occur and in some rare cases result in death.
Who Is at Risk for Shoulder Dystocia?
Risk factors for shoulder dystocia include having shoulder dystocia in a prior pregnancy, fetal macrosomia, gestational diabetes, and excessive weight gain during pregnancy.
More Resources for Victims and Lawyers
- Overview of medical malpractice cases in Maryland
- Overview of typical birth injury claims
- Medical malpractice frequently asked questions
- Example shoulder dystocia lawsuits
- A Carroll County Maryland plaintiff alleges excessive traction
- Brachial plexus lawsuit after shoulder dystocia complication in Baltimore
- Another shoulder dystocia lawsuit in Baltimore